🎉 Affordable, Reliable & Efficient Medical Billing Services at Just 2.99% + FREE Value Added Services!🎉 Affordable, Reliable & Efficient Medical Billing Services at Just 2.99% + FREE Value Added Services! | 🎉 Affordable, Reliable & Efficient Medical Billing Services at Just 2.99% + FREE Value Added Services! | 🎉 Affordable, Reliable & Efficient Medical Billing Services at Just 2.99% + FREE Value Added Services! |
Summit RCM helps maximize your revenue and streamline billing.
🎉 Thank You!
Your email was submitted successfully.
CPT 64493–64495: Lumbar Medial Branch Block (Facet) Coding Made Easy
By Summit RCM |
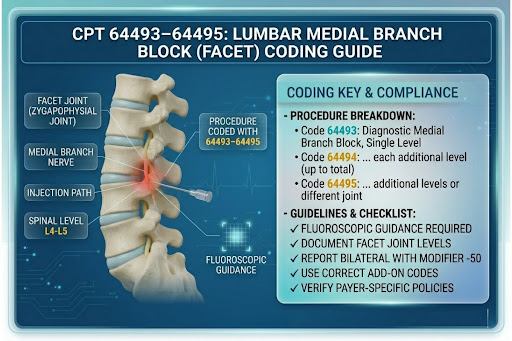
CPT 64493–64495 are used to bill lumbar medial branch block procedures. These injections target the nerves that carry pain signals from the facet joints in the lower spine.
Many practices unknowingly underbill or fail to meet payer requirements. Even a single coding error in 64493–64495 can cost your practice thousands in lost revenue. Understanding how these codes work is essential for accurate billing and compliance.
In this guide, you’ll learn how to use CPT 64493–64495 correctly, avoid common errors, and improve reimbursement outcomes for your practice.
A lumbar medial branch block (MBB) is a diagnostic or therapeutic injection used to identify or relieve pain originating from the facet joints in the lumbar spine.
Key Purpose:
Diagnose facet joint pain
Provide temporary pain relief
Determine if a patient is a candidate for radiofrequency ablation (RFA)
How It Works:
The medial branch nerves transmit pain signals from the facet joints to the brain. By injecting a local anesthetic (sometimes with a steroid), physicians can temporarily block these signals.
Medial branch blocks are often used as a diagnostic step before more advanced treatments like radiofrequency ablation (RFA).
Facet Joint Injection vs Medial Branch Block
This is a common area of confusion in pain management coding. Using the wrong code can lead to denials or compliance issues.
Category
Facet Joint Injection
Medial Branch Block
Target Area
Injected directly into the facet joint
Targets the medial branch nerves supplying the joint
Purpose
Treat inflammation within the joint
Block pain signals from the joint
CPT Codes
64490–64492
64493–64495
Procedure Focus
Joint structure
Nerve supply
Identification
Injection is placed inside the joint
Injection is placed near the medial branch nerve
CPT 64493–64495 Code Breakdown
CPT Code
Description
64493
Injection, diagnostic or therapeutic agent, paravertebral facet joint (or nerves innervating that joint), lumbar or sacral; single level
64494
Second level (add-on code)
64495
Third level (add-on code)
Understanding how each code works is key to accurate billing. These codes are based on the number of levels treated rather than the number of injections.
What Counts as a “Level”?
A level refers to a facet joint segment, not the number of needle insertions.
Example:
L3–L4 = 1 level
L4–L5 = another level
L5–S1 = another level
If a physician performs injections at:
L4–L5 → use 64493
L4–L5 and L5–S1 → use 64493 + 64494
L4–L5, L5–S1, and L3–L4 → use 64493 + 64494 + 64495
Getting these right is critical. Incorrect level reporting is one of the biggest reasons for claim denials.
Lumbar Medial Branch Block Billing Guidelines
Accurate coding requires more than selecting the correct CPT code. You must follow specific guidelines to ensure compliance and proper reimbursement.
1. Add-On Code Rules
64494 and 64495 cannot be billed alone
They must always be billed with 64493
2. Bilateral Procedures
If injections are performed on both sides (left and right) at the same level:
Report one CPT code
Add modifier -50 (bilateral)
Example:
Bilateral L4–L5 injection → 64493-50
3. Imaging Guidance Is Included
Fluoroscopy or CT guidance is included in 64493–64495
Do NOT bill separately for imaging (e.g., 77003)
4. Multiple Levels vs Multiple Injections
Even if multiple injections are given at the same level (e.g., targeting different nerves), it still counts as one level.
5. Global Period
These procedures typically have a 0-day global period
Follow-up visits can often be billed separately (if medically necessary)
Documentation Requirements
Accurate documentation is essential for claim approval. Even correctly coded claims can be denied if documentation is incomplete or unclear.
Errors in CPT 64493–64495 coding are common and can directly impact reimbursement. Avoiding these mistakes is key to reducing denials and improving cash flow.
1. Incorrect Level Counting
Many coders confuse injections with levels. Always count facet joint levels, not the number of needle insertions.
2. Billing Add-On Codes Alone
Codes 64494 and 64495 are add-on codes. They must always be billed with 64493.
3. Incorrect Modifier Usage
Using the wrong modifier can delay or deny claims. Follow payer guidelines for -50 vs LT/RT.
4. Billing Imaging Separately
Fluoroscopy is often billed incorrectly. Imaging is already included in these codes.
5. Weak Documentation
Incomplete documentation fails medical necessity checks. Include levels, laterality, diagnosis, and patient response.
6. Wrong Diagnosis Code
Using unrelated diagnoses can result in denial. Ensure the diagnosis supports facet joint pain.
7. Duplicate Billing
Billing the same level more than once is a common error. Each level should be reported only once per session.
Avoiding these mistakes improves claim acceptance, reduces delays, and increases overall reimbursement.
Tips to Maximize Reimbursement
Maximizing reimbursement for CPT 64493–64495 requires accuracy, consistency, and a proactive billing approach.
1. Verify Eligibility and Authorization
Always confirm:
Patient insurance coverage
Prior authorization requirements
Payer-specific rules
This helps prevent avoidable denials.
2. Code Correct Levels Every Time
Ensure the correct number of levels is billed.
One level = 64493
Additional levels = add-on codes
Undercoding or overcoding directly affects revenue.
3. Use Modifiers Correctly
Apply the right modifier based on payer requirements:
-50 for bilateral
LT/RT when required
Incorrect modifiers can delay payments.
4. Strengthen Documentation
Clear and detailed documentation supports:
Medical necessity
Faster approvals
Reduced audit risk
5. Track Procedure Outcomes
Document pain relief after injections. This is important for:
Future approvals
RFA eligibility
Compliance with payer policies
Tracking outcomes is critical, especially for RFA eligibility.
6. Monitor Denials and Take Action
Regularly review denied claims and identify patterns. Fix issues quickly to avoid repeated revenue loss.
Audit your claims regularly to catch and resolve issues early.
7. Stay Updated with Payer Guidelines
Medicare and commercial insurers frequently update their policies. Staying compliant helps avoid unnecessary rejections.
Q1: Can I bill 64493 multiple times for the same level?
No. One level = one unit, regardless of the number of injections.
Q2: Can I bill left and right separately?
Depends on payer:
Some require -50
Others prefer LT/RT
Q3: Is prior authorization required?
Often yes—especially for Medicare Advantage and private insurers.
Q4: What if more than 3 levels are treated?
Most payers do not reimburse beyond 3 levels
Optimize Your Medical Billing with Summit RCM
CPT 64493–64495 are essential for billing lumbar medial branch block procedures. Practices that follow structured coding and billing processes achieve better reimbursement, fewer claim issues, and improved cash flow.
Summit RCM provides reliable and efficient medical billing services designed to reduce denials, improve reimbursement, and streamline your entire revenue cycle. Our team specializes in accurate coding, compliance, and end-to-end billing support, allowing your practice to focus on patient care.
Get a free billing audit and identify hidden revenue leaks in your practice within 24–48 hours.
.png)