Radiofrequency Ablation (RFA) of lumbar facet joints is a widely performed interventional pain management procedure used to provide long-term relief for chronic lower back pain. While clinically effective, coding for lumbar facet RFA using CPT 64635 and 64636 is often misunderstood, leading to denials, underpayments, and compliance risks.
This guide explains how to code lumbar facet RFA accurately, including levels, sides, and session rules, to ensure compliance and maximize reimbursement.
Understanding Lumbar Facet RFA
Lumbar facet RFA is a therapeutic procedure that targets the medial branch nerves supplying facet joints in the lumbar spine. Using radiofrequency energy, the physician creates thermal lesions to interrupt pain signals.
Unlike diagnostic procedures such as medial branch blocks (MBB), RFA is performed only after confirming the pain source.
Key Purpose of RFA
- Provide long-term pain relief (6–12 months)
- Reduce reliance on medications
- Improve mobility and quality of life
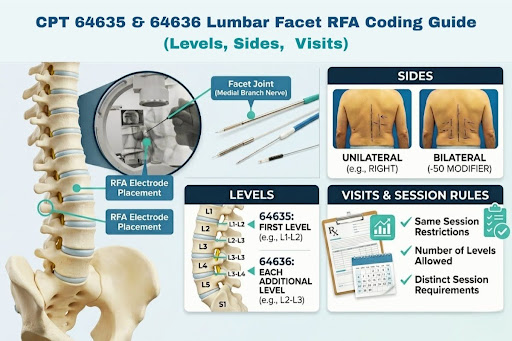
CPT Codes Overview: 64635 & 64636
Understanding the structure of these codes is critical.
64635 – Destruction by neurolytic agent (radiofrequency), lumbar or sacral, single facet joint (first level)
+64636 – Each additional facet joint (add-on code)
Key Coding Principle
These codes are reported based on facet joint levels, not:
- Number of nerves treated
- Number of needles used
- Number of lesions created
First Level vs Additional Levels
- Use 64635 once per session for the first facet joint level
- Use +64636 for each additional level treated
Important Notes
- 64636 is an add-on code and cannot be billed alone
- Do not report more than 3 levels per region (payer dependent)
- Always confirm levels before assigning codes
Facet Joint Anatomy (Critical for Coding)
Accurate coding depends on understanding how facet joints are innervated.
Code by Joint, Not Nerves
Always code based on facet joint levels, not:
- Medial branch nerves
- Number of lesions
- Number of needles
One Facet Joint = One Level
Each facet joint exists between two vertebrae:
- L3–L4 = 1 level
- L4–L5 = 1 level
Two Nerves Still Equal One Level
Two medial branch nerves supply each joint:
- One from the same level
- One from the level above
Even if both nerves are ablated, it still counts as one level
Example 1.
Documentation:
“RFA performed at L3, L4 medial branches”
Interpretation:
L3 + L4 nerves → L4–L5 joint = 1 level
Example 2.
Documentation:
“RFA at L3, L4, L5 medial branches”
Interpretation:
L3–L4 and L4–L5 = 2 levels
Translate documentation into facet joint levels first, then assign CPT codes.
Coding for Laterality (Sides)
In addition to identifying levels, correct coding for CPT 64635 and 64636 also depends on accurately reporting laterality—whether the procedure was performed on the right side, left side, or both.
Unilateral Procedures
If RFA is performed on only one side:
Right side → RT modifier
Left side → LT modifier
Bilateral Procedures
If the same levels are treated on both sides, the procedure is considered bilateral.
There are two common ways to report this:
Option 1: RT and LT Modifiers (Preferred)
- Report each side separately
- This is accepted by most payers
Example:
64635 RT
64635 LT
Option 2: Modifier 50 (Payer Dependent)
- Some payers allow modifier 50 for bilateral procedures
- Always verify payer guidelines before using
Multiple Levels with Laterality
If multiple levels are treated bilaterally:
Example:
L3–L4 and L4–L5 on both sides
Coding:
64635 RT
64635 LT
+64636 RT
+64636 LT
Always clearly identify the side(s) treated and apply modifiers correctly based on payer requirements.
Coding by Visits and Sessions
Understanding how CPT 64635 and 64636 apply across visits and sessions is essential for accurate billing and avoiding duplicate or denied claims.
One Session = One Coding Event
Each procedure session is coded independently, even if the same patient returns for additional treatments.
- Codes are assigned per date of service
- Do not combine multiple visits into a single claim
Same-Day Rules
- Report codes based on all levels treated in that single session
- Do not split levels across multiple claims for the same day
Staged Procedures (Multiple Visits)
In some cases, physicians treat different levels or sides across multiple visits.
Example:
Visit 1: Right side L3–L4
Visit 2: Left side L3–L4
Each visit is coded separately with appropriate modifiers.
Repeat RFA Procedures
RFA may be repeated if:
- Pain returns
- Previous procedure provided relief
Requirements:
- Document prior success
- Justify medical necessity
Important Considerations
- Do not bill the same level again without medical necessity
- Ensure documentation clearly supports each session
- Follow payer frequency guidelines
Code per session, per visit, and ensure each claim is supported by proper documentation and medical necessity.
Documentation Requirements
Proper documentation is essential for reimbursement.
Key Elements to Include
Ensure the procedure note clearly documents:
- Facet joint levels treated
- Laterality (right, left, or bilateral)
- Procedure performed (radiofrequency ablation/neurotomy)
- Imaging guidance used (fluoroscopy or CT)
- Technique details (lesioning, probe placement, etc.)
Prior Diagnostic Requirement
Most payers require evidence of prior medial branch block (MBB) before RFA.
Documentation should include:
- Number of prior MBBs performed
- Percentage of pain relief achieved
- Duration of relief
- Consistency of pain pattern
Medical Necessity
To support reimbursement, documentation must show:
- Chronic pain not responding to conservative treatment
- Functional limitations
- Justification for proceeding with RFA
Strong, detailed documentation is essential to justify the procedure and ensure successful reimbursement.
Step-by-Step Coding Workflow
Step 1: Confirm Procedure Type
Ensure documentation clearly states:
Radiofrequency ablation
Neurotomy / lesioning
Avoid confusion with injections (MBB).
Step 2: Identify Levels Treated
Translate documentation into joint levels.
Example:
“Ablation at L3, L4, L5 medial branches”
Equals:
L3–L4 joint
L4–L5 joint
= 2 levels
Step 3: Assign CPT Codes
First level → 64635
Additional levels → +64636
Example
Procedure:
L3–L4 and L4–L5
Coding:
64635
+64636
Step 4: Determine Laterality (Sides)
RFA can be:
Unilateral (one side)
Bilateral (both sides)
Modifier Usage
| Scenario |
Coding |
| Right side only |
64635 RT |
| Left side only |
64635 LT |
| Bilateral |
RT/LT or modifier 50 (payer dependent) |
Many payers prefer:
Separate line items instead of modifier 50
Real-World Coding Examples
Understanding CPT 64635 and 64636 becomes much easier when applied to real scenarios. Below are common cases you’ll encounter in practice.
Example 1: Single-Level Unilateral RFA
Procedure:
RFA performed at L4–L5 (right side)
Coding:
64635 RT
Example 2: Two-Level Unilateral RFA
Procedure:
RFA at L3–L4 and L4–L5 (left side)
Coding:
64635 LT
+64636 LT
Example 3: Single-Level Bilateral RFA
Procedure:
RFA at L4–L5 on both sides
Coding (preferred method):
64635 RT
64635 LT
Example 4: Two-Level Bilateral RFA
Procedure:
RFA at L3–L4 and L4–L5 on both sides
Coding:
64635 RT
64635 LT
+64636 RT
+64636 LT
Example 5: Interpreting Nerve-Based Documentation
Procedure Note:
“Ablation performed at L3, L4, L5 medial branches”
Correct Interpretation:
L3–L4 and L4–L5 = 2 levels
Coding:
64635
+64636
Always convert documentation into facet joint levels first, then apply CPT codes and modifiers accurately.
Common Coding Mistakes to Avoid
Even experienced coders make errors when billing CPT 64635 and 64636, often leading to denials or compliance issues.
1. Coding Based on Nerves Instead of Levels
- Counting medial branch nerves instead of facet joint levels
- Assuming more nerves = more billable levels
2. Incorrect Level Interpretation
- Misreading documentation like “L3, L4, L5 medial branches”
- Overcoding levels due to misunderstanding anatomy
3. Missing or Incorrect Modifiers
- Not applying RT/LT for unilateral procedures
- Incorrect use of modifier 50 for bilateral cases
4. Billing Unsupported Levels
- Reporting more than 3 levels per region
- Billing levels not clearly documented
5. Ignoring Visit-Based Rules
- Combining multiple sessions into one claim
- Billing repeat procedures without proper justification
6. Incomplete Documentation
- Missing prior MBB details
- No pain relief percentage documented
- Unclear procedure notes
Most denials occur due to level confusion, modifier errors, or weak documentation—addressing these areas improves claim success.
Revenue Optimization Tips
Maximizing reimbursement for CPT 64635 and 64636 requires more than correct coding—it involves consistency, documentation quality, and payer awareness.
Ensure Accurate Level Reporting
- Verify levels directly from procedure notes
- Avoid undercoding or overcoding due to misinterpretation
Use Modifiers Correctly
- Apply RT/LT consistently
- Follow payer preference for bilateral billing
To better understand how modifiers impact reimbursement accuracy, explore our guide on the Role of Modifiers in Wound Care Coding.
Strengthen Documentation
- Clearly state levels and sides
- Include prior MBB results and pain relief %
- Ensure medical necessity is well documented
Follow Payer Guidelines
- Check requirements for diagnostic blocks
- Confirm allowed number of levels
- Stay updated on payer-specific rules
Monitor Denials
- Track common denial reasons
- Adjust workflows to prevent repeat issues
Accurate coding + strong documentation + payer alignment = higher reimbursement and fewer denials
To see how outsourcing can improve efficiency and reduce costs, check out our guide on the Benefits of Virtual Medical Billing Assistants.
FAQs: CPT 64635 & 64636 Coding
1. How many levels can be billed in one session?
Most payers allow billing for up to 3 facet joint levels per region. Billing beyond this may lead to denials unless medically justified.
2. How do you code bilateral procedures?
- Use RT and LT modifiers on separate line items (preferred by most payers)
- Modifier 50 may be used if allowed by the payer
3. What if documentation lists only nerves?
You must convert nerve documentation into facet joint levels before coding.
4. Can RFA be repeated?
Yes, if:
- Pain returns
- Prior procedure provided relief
- Medical necessity is documented
5. Are multiple visits billed separately?
Yes. Each session is coded based on its date of service and documented levels.
Simplify Your RFA Coding and Maximize Revenue with Summit RCM
Accurate coding for CPT 64635 and 64636 depends on correct facet joint level counting, proper modifier usage, and strong documentation. Getting these elements right helps reduce denials, ensure compliance, and maintain consistent reimbursement.
Partner with Summit RCM for comprehensive Medical revenue cycle management services that streamline your billing operations, reduce claim rejections, and improve cash flow. From coding to collections, their team ensures your entire revenue cycle runs efficiently.
Contact Summit RCM today to optimize your revenue cycle and maximize profitability.
.png)