In selective debridement, CPT 97597 and CPT 97598 are two codes that often get mixed up. They
are performed in the same setting, used for the same type of service, and appear side-by-side on
many claims. But the way each code works is very different.
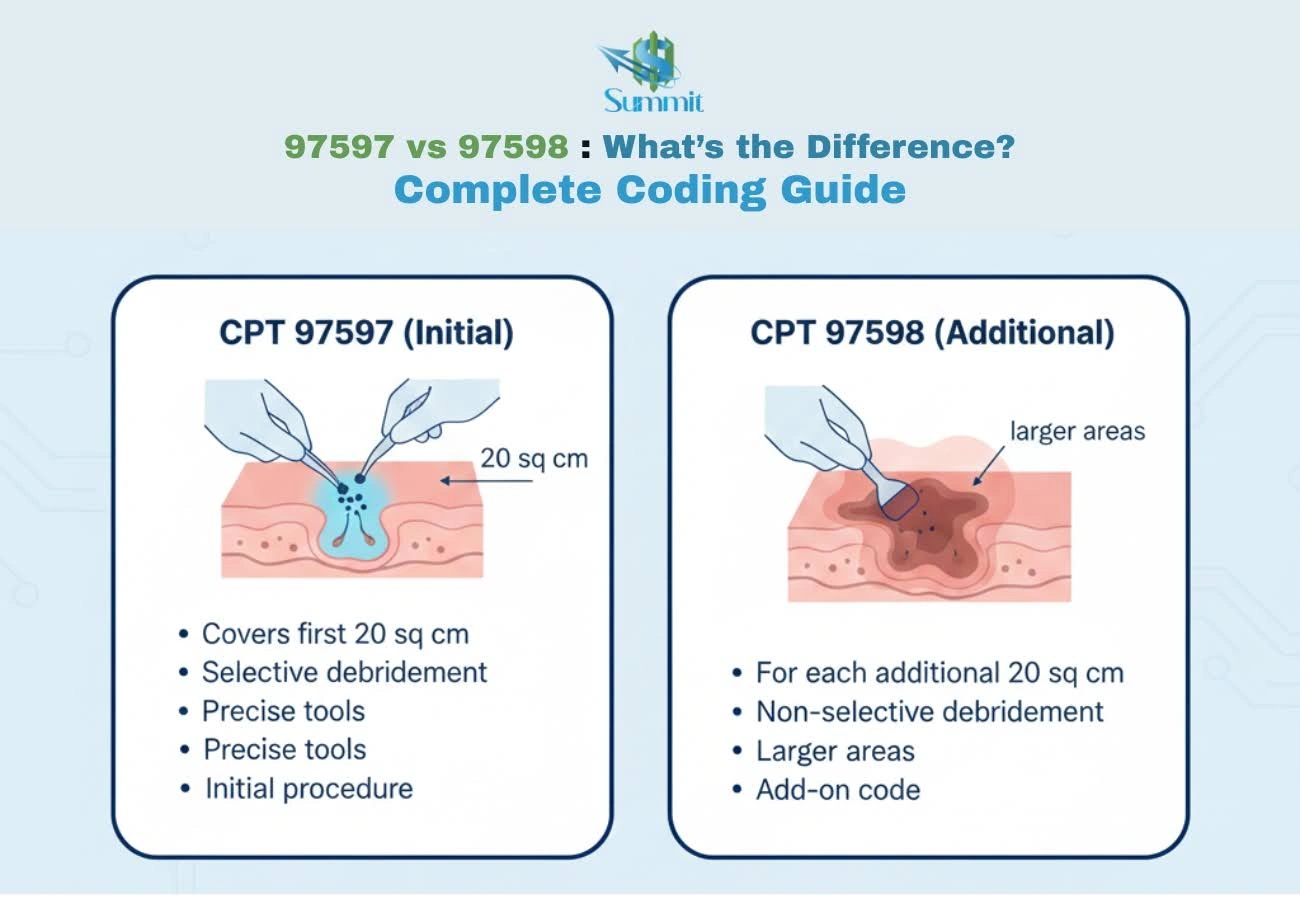
CPT 97597 covers the initial 20 sq cm of selective debridement. CPT 97598 is an add-on code for
each additional 20 sq cm or part of it treated during the same session. So when a wound exceeds
20 sq cm, you bill 97597 once and add 97598 as many times as needed based on the total area.
This guide simplifies 97597 vs 97598 and gives you the exact rules for using each code, ensuring
accurate selective debridement coding and cleaner claims.
What is CPT 97597 – Debridement (First 20
sq cm)
CPT 97597 is used for selective debridement of devitalized tissue from an open wound measuring 20
sq cm or less. It covers the initial portion of the service performed during a single session.
When providers use it:
This code is commonly used for treating wounds that require removal of slough, biofilm, necrotic
tissue, or foreign material to promote healing. It is often seen in outpatient wound care,
podiatry, primary care, and hospital-based wound centers.
Techniques included:
Selective debridement under 97597 may involve:
- Scissors
- Scalpels
- Forceps
- Tweezers
- Enzymatic agents
- High-pressure irrigation (when used to remove devitalized tissue)
Documentation requirements:
For accurate medical billing, documentation should include:
- Wound type and anatomical location
- Total surface area treated (in sq cm)
- Specific technique used for debridement
- Description of devitalized tissue removed
- Patient tolerance and wound appearance before/after treatment
What is CPT 97598 – Add-On Code
CPT 97598 is an add-on code used for selective debridement beyond the initial 20 sq cm. It
applies to each additional 20 sq cm or part thereof treated during the same session.
How it complements 97597:
97598 cannot be billed alone. It is always billed in addition to 97597 when the wound area
exceeds 20 sq cm. This makes it the correct way to code larger or multiple wounds with a
combined area over the base code threshold.
When and why it should be added:
Use 97598 when:
- The total wound area treated is greater than 20 sq cm
- Multiple wounds collectively exceed 20 sq cm
- Additional debridement work is performed beyond the initial unit covered by 97597
Documentation requirements:
Documentation must clearly show:
- Total cumulative wound surface area debrided
- Justification for additional units
- Techniques used for the extended area
- Confirmation that the service occurred in the same session as 97597
Key Differences Between CPT 97597
and CPT
97598
CPT 97597 and 97598 work together in selective debridement, but each code represents a different
part of the service. The table below shows the key distinctions you need to know:
| Feature |
CPT 97597 |
CPT 97598 |
| Code Type |
Stand-alone code |
Add-on code (cannot be billed alone) |
| Purpose |
Covers the initial selective debridement |
Covers additional selective debridement beyond the first 20 sq cm |
| Surface Area |
First 20 sq cm |
Each additional 20 sq cm or part thereof |
| Billing Frequency |
Billed once per session |
Billed in units based on extra wound area |
| When Use |
Any wound ≤20 sq cm, or the first 20 sq cm of a larger wound |
When the total treated area exceeds 20 sq cm |
| Applicability |
Can be billed alone |
Must be billed with 97597 in the same session |
| Multiple Wounds |
Covers the first 20 sq cm of combined wound areas |
Used when combined areas go beyond 20 sq cm |
How to Choose the Correct Code:
Step-by-Step
Selecting the right code for selective debridement starts with understanding the total wound area
treated and how much work is performed during the session. Once you know the wound size and
method used, choosing between CPT 97597 and 97598 becomes simple. Follow the steps below to code
accurately every time:
Step 1. Determine the wound type
Confirm that the service qualifies as selective debridement, not surgical debridement. Selective
techniques include scissors, forceps, scalpels, tweezers, or enzymatic/irrigation methods.
Step 2. Measure the total surface area
Add the surface area of all wounds treated with the same selective method during the session.
Calculate in square centimeters.
Step 3. Identify the first 20 sq cm (use 97597)
The first 20 sq cm of total wound area is always billed with CPT 97597. This code is billed once
per session.
Step 4. Calculate additional units (use 97598)
When the total treated area exceeds 20 sq cm, bill CPT 97598 for each additional 20 sq cm or any
part of it.
- Example: An extra 1–20 sq cm = 1 unit
- Example: An extra 21–40 sq cm = 2 units
Step 5. Apply proper modifiers if needed
Use modifiers when required by payer rules, especially for:
- Multiple wounds
- Different anatomical sites
- Distinct services performed in the same visit
- (Modifier usage varies by payer; always verify.)
Step 6. Confirm documentation support
Ensure the provider’s notes clearly include:
- Wound type and location
- Total surface area treated
- Debridement technique used
- Description of tissue removed
- Patient response
Accurate documentation is essential for clean claims and to justify any additional units
billed.
Common Coding Mistakes and How to Avoid Them
In wound care billing, correct
coding for debridement procedures can be challenging, especially when multiple wounds or
larger surface areas are involved. Here are the most frequent errors and how to prevent them.
1. Billing 97598 Without 97597
-
Mistake: Using 97598 alone.
-
Avoid it: Always pair 97598 with 97597 in the same session. It is an add-on code and
cannot
stand alone.
2. Combining Different Debridement Types
-
Mistake: Adding selective and surgical debridement areas together.
-
Avoid it: Only combine wound areas treated with the same selective method. Surgical
debridement
must be coded separately.
3. Incorrect Surface Area Calculations
-
Mistake: Measuring wounds incorrectly or not converting to square centimeters.
-
Avoid it: Document the exact size of each wound and add the areas accurately. Convert
measurements to sq cm when needed.
4. Missing Documentation for Additional Units
Mistake: Billing 97598 units without clear notes supporting the extra area treated.
Avoid it: Documentation must state:
- Total area debrided
- Additional area beyond 20 sq cm
- Techniques used
Clear documentation = clean claims.
5. Using These Codes for Non-Selective Debridement
-
Mistake: Applying 97597/97598 to sharp surgical debridement or excisional procedures.
-
Avoid it: These codes are only for selective debridement. Surgical methods require the
11042–11047 series.
6. Overlooking Modifier Requirements
-
Mistake: Not using modifiers when working on different anatomical sites.
-
Avoid it: Apply modifiers (payer-dependent) when treating separate areas or when multiple
procedures occur in the same session.
7. Billing Multiple Units of 97597
-
Mistake: Using 97597 more than once per session.
-
Avoid it: Bill 97597 once only. Additional area always falls under 97598.
Real-World Coding Examples of Wound Care
Billing
These examples show how to apply CPT 97597 and 97598 based on total wound surface area and the
amount of selective debridement performed.
Example 1: Single Small Wound
-
Wound size: 18 sq cm
-
Coding: 97597 only
-
Why: Total treated area is within the first 20 sq cm, so no add-on code is needed.
Example 2: Larger Wound Over 20 sq cm
Wound size: 34 sq cm
Coding: 97597 + 1 unit of 97598
Why:
- First 20 sq cm → 97597
- Remaining 14 sq cm → one unit of 97598
Example 3: Large Combined Surface Area
Wound sizes:
- Wound #1: 22 sq cm
- Wound #2: 25 sq cm
Total treated area: 47 sq cm
Coding: 97597 + 2 units of 97598
Why:
- First 20 sq cm → 97597
- Remaining 27 sq cm → two units of 97598 (covers 21–40 sq cm)
Example 4: Multiple Wounds, Different Techniques
Wound sizes:
- Wound #1: 18 sq cm (selective)
- Wound #2: 22 sq cm (surgical debridement)
Coding:
- Selective wound → 97597
- Surgical wound → 11042-11047 series (not 97598)
Why:
You cannot combine areas from different debridement types. Each method must be coded separately.
Payer and Billing Considerations
for CPT 97597
and 97598
Payer rules for CPT 97597 and 97598 can vary, and understanding these differences is key to
avoiding denials and ensuring accurate reimbursement. Here are the most important billing
considerations to keep in mind.
1. Medicare Guidelines
Medicare typically follows CPT rules closely for selective debridement.
Key points:
- 97597 billed once per session
- 97598 billed in units for additional wound surface area
- Documentation must clearly support the total area treated and the method used
Always check your local Medicare Administrative Contractor (MAC) for policy updates.
2. Commercial Payer Variations
Private insurers may have additional requirements. Common differences include:
- Requests for more detailed wound measurements
- Specific expectations for wound descriptions (e.g., tissue type, percentage removed)
- Prior authorization rules for repeated debridement sessions
Verifying payer-specific policies helps prevent unnecessary denials.
3. Medically Unlikely Edits (MUEs)
CMS MUEs limit how many units of 97598 can be billed per date of service.
- Exceeding the MUE may trigger an automatic denial
- Some payers allow appeals with proper documentation
Always confirm that your total units fall within payer limits.
4. NCCI Bundling Rules
National Correct Coding Initiative (NCCI) edits govern which codes can be billed together.
Important reminders:
- 97597/97598 cannot be billed with surgical debridement codes (11042–11047) for the same
wound
- Some evaluation and management (E/M) services may require modifiers when performed on the
same day
Check for bundling edits before submitting claims to keep your claims
clean and compliant.
5. Modifier Requirements (Payer-Specific)
Modifiers may be required when:
- Treating separate anatomical sites
- Performing distinct services
- Billing multiple procedures on the same date
Common modifiers include 59, XS, or payer-preferred alternatives.
Always follow your payer’s modifier guidelines.
6. Frequency Limits
Some payers limit how often selective debridement can be billed.
Examples:
- Weekly frequency limits
- Medical necessity reviews for recurring visits
- Requirements for showing clinical improvement over time
Ensure that documentation supports the ongoing need for treatment.
Level Up Your Wound Care Coding Accuracy
with
Summit RCM
Understanding CPT 97597 and 97598 is essential for accurate coding, cleaner claims, and reliable
reimbursement. Practices looking to improve accuracy and strengthen reimbursement performance
can rely on Summit RCM for expert support.
Our team specializes in wound care
billing and delivers full-service revenue cycle
solutions designed to enhance efficiency and boost profitability.
Improve accuracy and boost reimbursement. Contact Summit RCM today.
.png)